
Central Retinal Vein Occlusion in a Young Woman with Diabetes and Hypertension after mRNA-Based COVID-19 Vaccination—A Case Report and Brief Review of the Literature

Abstract
:1. Introduction
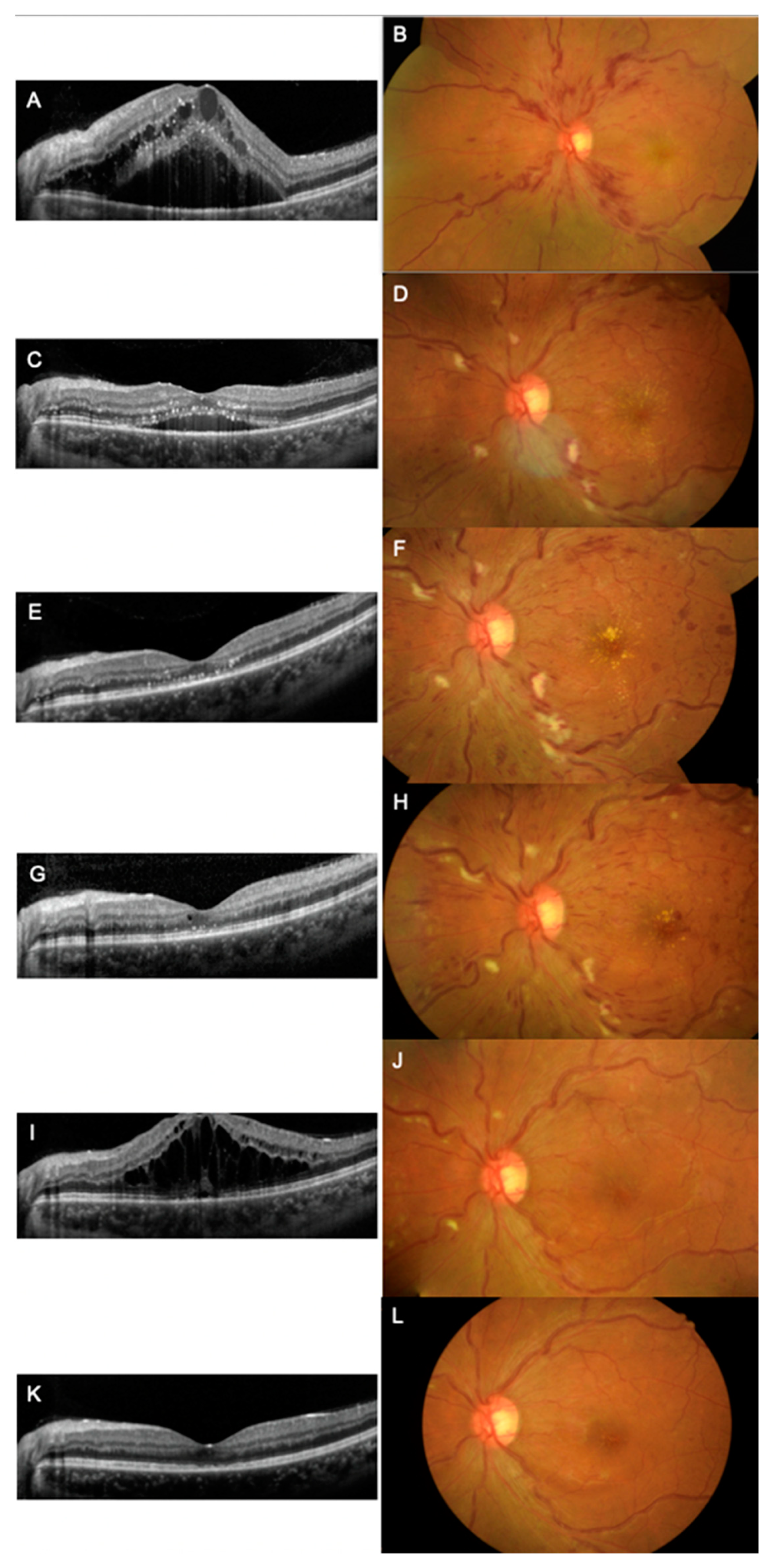
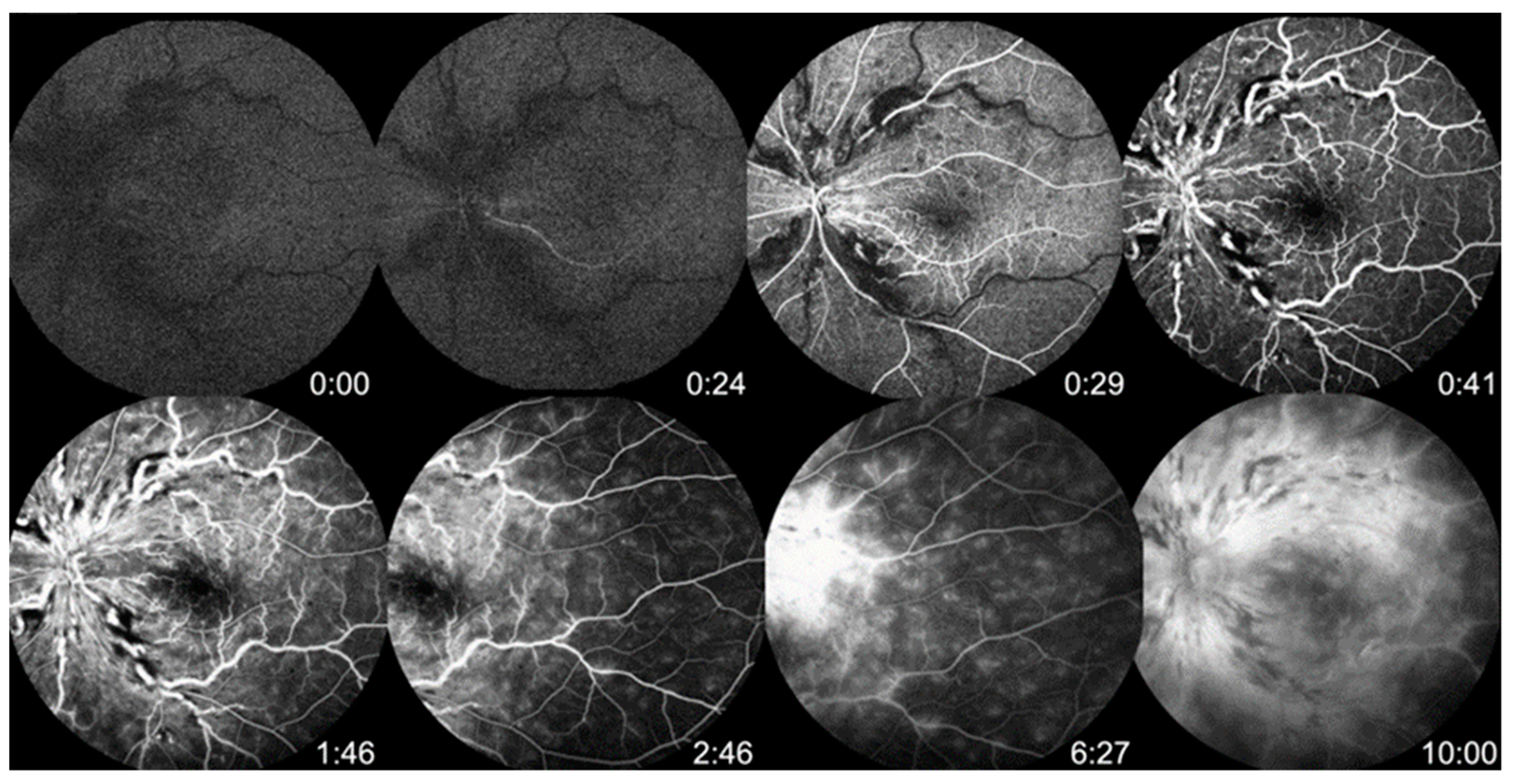
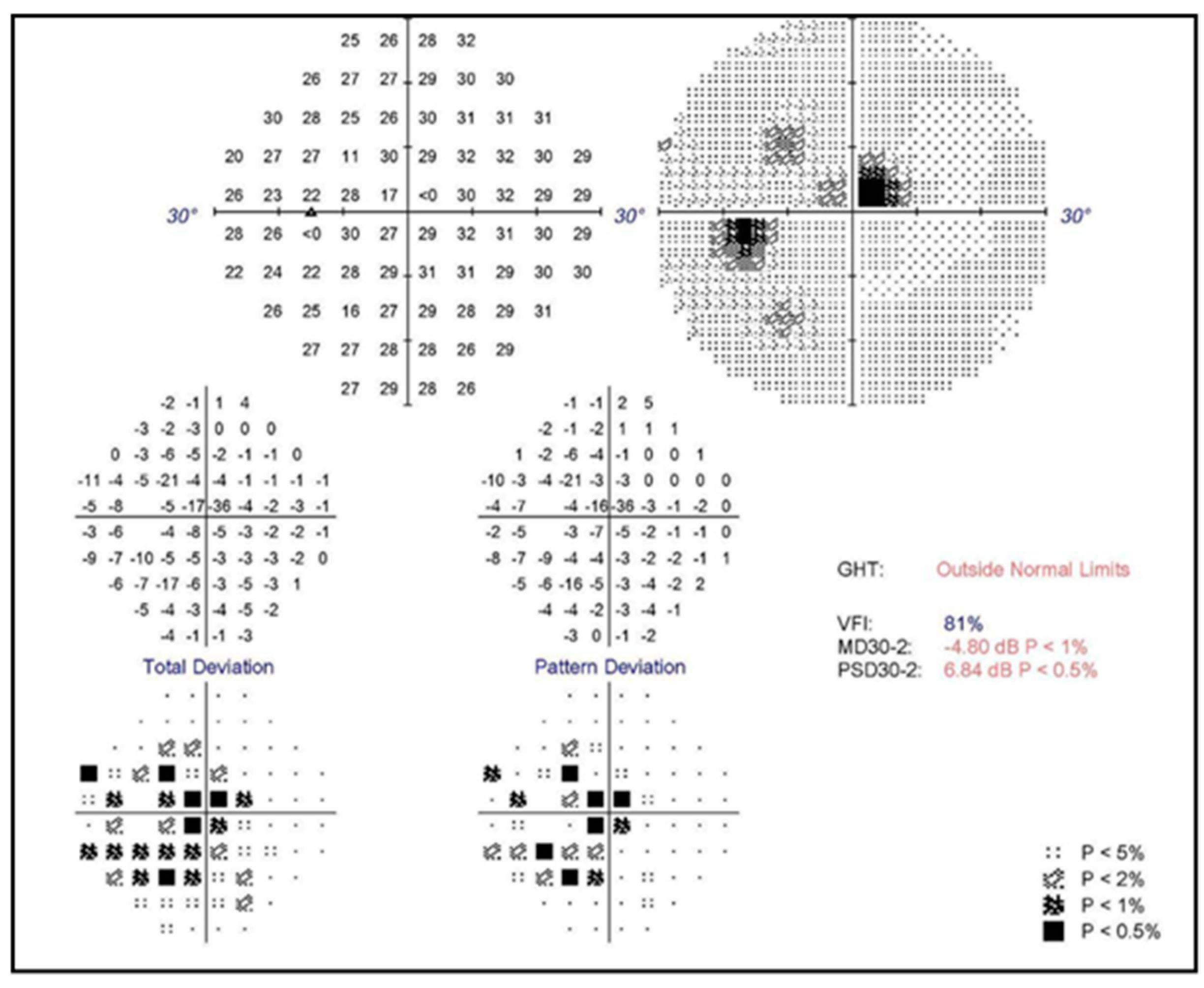
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thomas, S.J.; Moreira, E.D., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Heath, P.T.; Galiza, E.P.; Baxter, D.N.; Boffito, M.; Browne, D.; Burns, F.; Chadwick, D.R.; Clark, R.; Cosgrove, C.; Galloway, J.; et al. Safety and Efficacy of NVX-CoV2373 Covid-19 Vaccine. N. Engl. J. Med. 2021, 385, 1172–1183. [Google Scholar] [CrossRef] [PubMed]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Van Dromme, I.; Spiessens, B.; et al. Final Analysis of Efficacy and Safety of Single-Dose Ad26.COV2.S. N. Engl. J. Med. 2022, 386, 847–860. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- World Health Organization. COVID-19 Vaccines with WHO Emergency Use Listing. Available online: https://extranet.who.int/pqweb/vaccines/vaccinescovid-19-vaccine-eul-issued (accessed on 16 July 2022).
- Ng, X.L.; Betzler, B.K.; Ng, S.; Chee, S.P.; Rajamani, L.; Singhal, A.; Rousselot, A.; Pavesio, C.E.; Gupta, V.; de Smet, M.D.; et al. The Eye of the Storm: COVID-19 Vaccination and the Eye. Ophthalmol. Ther. 2022, 11, 81–100. [Google Scholar] [CrossRef]
- Lee, Y.K.; Huang, Y.H. Ocular Manifestations after Receiving COVID-19 Vaccine: A Systematic Review. Vaccines 2021, 9, 1404. [Google Scholar] [CrossRef]
- Lin, T.P.H.; Ko, C.N.; Zheng, K.; Lai, K.H.W.; Wong, R.L.M.; Lee, A.; Zhang, S.; Huang, S.S.; Wan, K.H.; Lam, D.S.C. COVID-19: Update on Its Ocular Involvements, and Complications from Its Treatments and Vaccinations. Asia Pac. J. Ophthalmol. 2021, 10, 521–529. [Google Scholar] [CrossRef]
- Ng, X.L.; Betzler, B.K.; Testi, I.; Ho, S.L.; Tien, M.; Ngo, W.K.; Zierhut, M.; Chee, S.P.; Gupta, V.; Pavesio, C.E.; et al. Ocular Adverse Events After COVID-19 Vaccination. Ocul. Immunol. Inflamm. 2021, 29, 1216–1224. [Google Scholar] [CrossRef]
- Song, P.; Xu, Y.; Zha, M.; Zhang, Y.; Rudan, I. Global epidemiology of retinal vein occlusion: A systematic review and meta-analysis of prevalence, incidence, and risk factors. J. Glob. Health 2019, 9, 010427. [Google Scholar] [CrossRef]
- Ip, M.; Hendrick, A. Retinal Vein Occlusion Review. Asia Pac. J. Ophthalmol. 2018, 7, 40–45. [Google Scholar] [CrossRef]
- Ophthalmologists, T.R.C.o. Retinal Vein Occlusion (RVO) Guidelines; The Royal College of Ophthalmologists: London, UK, 2015. [Google Scholar]
- Klein, R.; Klein, B.E.; Moss, S.E.; Meuer, S.M. The epidemiology of retinal vein occlusion: The Beaver Dam Eye Study. Trans. Am. Ophthalmol. Soc. 2000, 98, 133–141, discussion 141–133. [Google Scholar] [PubMed]
- Rogers, S.; McIntosh, R.L.; Cheung, N.; Lim, L.; Wang, J.J.; Mitchell, P.; Kowalski, J.W.; Nguyen, H.; Wong, T.Y. The prevalence of retinal vein occlusion: Pooled data from population studies from the United States, Europe, Asia, and Australia. Ophthalmology 2010, 117, 313–319.e311. [Google Scholar] [CrossRef]
- Bialasiewicz, A.A.; Farah-Diab, M.S.; Mebarki, H.T. Central retinal vein occlusion occurring immediately after 2nd dose of mRNA SARS-CoV-2 vaccine. Int. Ophthalmol. 2021, 41, 3889–3892. [Google Scholar] [CrossRef]
- Priluck, A.Z.; Arevalo, J.F.; Pandit, R.R. Ischemic retinal events after COVID-19 vaccination. Am. J. Ophthalmol. Case Rep. 2022, 26, 101540. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Nagasato, D.; Nakakura, S.; Tanabe, H.; Nagasawa, T.; Wakuda, H.; Imada, Y.; Mitamura, Y.; Tabuchi, H. Exacerbation of branch retinal vein occlusion post SARS-CoV2 vaccination: Case reports. Medicine 2021, 100, e28236. [Google Scholar] [CrossRef]
- Peters, M.C.; Cheng, S.S.H.; Sharma, A.; Moloney, T.P. Retinal vein occlusion following COVID-19 vaccination. Clin. Exp. Ophthalmol. 2022, 50, 459–461. [Google Scholar] [CrossRef]
- Sugihara, K.; Kono, M.; Tanito, M. Branch Retinal Vein Occlusion after Messenger RNA-Based COVID-19 Vaccine. Case Rep. Ophthalmol. 2022, 13, 28–32. [Google Scholar] [CrossRef]
- Ikegami, Y.; Numaga, J.; Okano, N.; Fukuda, S.; Yamamoto, H.; Terada, Y. Combined central retinal artery and vein occlusion shortly after mRNA-SARS-CoV-2 vaccination. Qjm 2022, 114, 884–885. [Google Scholar] [CrossRef]
- Sacconi, R.; Simona, F.; Forte, P.; Querques, G. Retinal Vein Occlusion Following Two Doses of mRNA-1237 (Moderna) Immunization for SARS-Cov-2: A Case Report. Ophthalmol. Ther. 2022, 11, 453–458. [Google Scholar] [CrossRef]
- Park, H.S.; Byun, Y.; Byeon, S.H.; Kim, S.S.; Kim, Y.J.; Lee, C.S. Retinal Hemorrhage after SARS-CoV-2 Vaccination. J. Clin. Med. 2021, 10, 5705. [Google Scholar] [CrossRef]
- Sonawane, N.J.; Yadav, D.; Kota, A.R.; Singh, H.V. Central retinal vein occlusion post-COVID-19 vaccination. Indian. J. Ophthalmol. 2022, 70, 308–309. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Sankhala, K.K.; Bose, S.; Gallemore, R.P. Combined Central Retinal Artery and Vein Occlusion with Ischemic Optic Neuropathy After COVID-19 Vaccination. Int. Med. Case. Rep. J. 2022, 15, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Romano, D.; Morescalchi, F.; Romano, V.; Semeraro, F. COVID-19 AdenoviralVector Vaccine and Central Retinal Vein Occlusion. Ocul. Immunol. Inflamm. 2022, 30, 1286–1288. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C. Combined central retinal artery occlusion and vein occlusion with exudative retinal detachment following COVID-19 vaccination. Kaohsiung J. Med. Sci. 2022, 38, 1020–1021. [Google Scholar] [CrossRef]
- Vujosevic, S.; Limoli, C.; Romano, S.; Vitale, L.; Villani, E.; Nucci, P. Retinal vascular occlusion and SARS-CoV-2 vaccination. Graefes Arch. Clin. Exp. Ophthalmol. 2022, 260, 3455–3464. [Google Scholar] [CrossRef]
- Dutta Majumder, P.; Prakash, V.J. Retinal venous occlusion following COVID-19 vaccination: Report of a case after third dose and review of the literature. Indian J. Ophthalmol. 2022, 70, 2191–2194. [Google Scholar] [CrossRef]
- Pur, D.R.; Catherine Danielle Bursztyn, L.L.; Iordanous, Y. Branch retinal vein occlusion in a healthy young man following mRNA COVID-19 vaccination. Am. J. Ophthalmol. Case Rep. 2022, 26, 101445. [Google Scholar] [CrossRef]
- Endo, B.; Bahamon, S.; Martínez-Pulgarín, D.F. Central retinal vein occlusion after mRNA SARS-CoV-2 vaccination: A case report. Indian J. Ophthalmol. 2021, 69, 2865–2866. [Google Scholar] [CrossRef]
- Shah, P.P.; Gelnick, S.; Jonisch, J.; Verma, R. Central Retinal Vein Occlusion Following BNT162b2 (Pfizer-BioNTech) COVID-19 Messenger RNA Vaccine. Retin. Cases Brief Rep. 2021. [Google Scholar] [CrossRef]
- Sodhi, P.K.; Yadav, A.; Sharma, B.; Sharma, A.; Kumar, P. Central Retinal Vein Occlusion Following the First Dose of COVID Vaccine. Cureus 2022, 14, e25842. [Google Scholar] [CrossRef]
- Takacs, A.; Ecsedy, M.; Nagy, Z.Z. Possible COVID-19 MRNA Vaccine-Induced Case of Unilateral Central Retinal Vein Occlusion. Ocul. Immunol. Inflamm. 2022, 1–6. [Google Scholar] [CrossRef]
- Karageorgiou, G.; Chronopoulou, K.; Georgalas, I.; Kandarakis, S.; Tservakis, I.; Petrou, P. Branch retinal vein occlusion following ChAdOx1 nCoV-19 (Oxford-AstraZeneca) vaccine. Eur. J. Ophthalmol. 2022, 11206721221124651. [Google Scholar] [CrossRef]
- Nangia, P.; Prakash, V.J.; Dutta Majumder, P. Retinal venous occlusion in a child following Corbevax COVID-19 vaccination. Indian J. Ophthalmol. 2022, 70, 3713–3715. [Google Scholar] [CrossRef]
- Tanaka, H.; Nagasato, D.; Nakakura, S.; Nagasawa, T.; Wakuda, H.; Kurusu, A.; Mitamura, Y.; Tabuchi, H. Branch retinal vein occlusion post severe acute respiratory syndrome coronavirus 2 vaccination. Taiwan J. Ophthalmol. 2022, 12, 202–205. [Google Scholar] [CrossRef]
- Cunningham, E.T.; Moorthy, R.S.; Agarwal, M.; Smit, D.P.; Zierhut, M. Ocular Complications Following COVID-19 Vaccination—Coincidence, Correlation, or Causation? Ocul. Immunol. Inflamm. 2022, 30, 1031–1034. [Google Scholar] [CrossRef]
- Thiele, T.; Ulm, L.; Holtfreter, S.; Schönborn, L.; Kuhn, S.O.; Scheer, C.; Warkentin, T.E.; Bröker, B.M.; Becker, K.; Aurich, K.; et al. Frequency of positive anti-PF4/polyanion antibody tests after COVID-19 vaccination with ChAdOx1 nCoV-19 and BNT162b2. Blood 2021, 138, 299–303. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Laboratory Test | Results | Laboratory Test | Results |
|---|---|---|---|
| White Blood Cell(/μL) | 8350 | RPR | Non-Reactive |
| Urea N (mg/dL) | 7.6 | ANA | <1.40 |
| Creatinine (mg/dL) | 0.48 | RA factor (IU/mL) | <10.0 |
| Na (m mol/L) | 134 | PT (second) | 10.5 |
| K (m mol/L) | 3.7 | PTT (second) | 27.1 |
| SGOT (IU/L) | 18 | D-Dimer (mg/L FEU) | 0.19 |
| SGPT (IU/L) | 27 | Protein C (%) | 97 |
| CRP (mg/L) | 1.98 | Protein S (%) | 88 |
| ESR (mm/h) | 9 | Homocysteine (μmol/L) | 6.59 |
| *HbA1c (%) | 9.2 | Anti-cardiolipin antibody | negative |
| Cholesterol (mg/dL) | 148 | Anti-β2 glycoprotein-I antibody | negative |
| TG (mg/dL) | 8 | LAC (lupus anticoagulant) (ratio) | <1.2 |
| Study | Case | Vaccine | First Onset (day) | Age | Sex | Risk Factors | Diagnosis | Management | Visual Acuity (Initial→Final) |
|---|---|---|---|---|---|---|---|---|---|
| Priluck et al. (Apr. 22) [17] | 1 | 2nd mRNA-1273 | - | 57 | F | HTN | BRVO | Aflibercept monthly for 6 months | 20/30->20/25 |
| Tanaka et al. (Nov. 21) [18] | 2 | 2nd BNT162b2 | 1 R | 71 | F | History of BRVO | BRVO | Aflibercept*1 | 20/30->20/20 |
| 1st BNT162b2 | 1 R | 72 | M | History of BRVO | BRVO | Ranibizumab*2 | 20/25->20/25 | ||
| Peters et al. (Jan. 22) [19] | 5 | 1st AZD1222 | 2 | 71 | M | Unremarkable | BRVO | Bevacizumab (monthly) | 6/60 |
| 1st AZD1222 | 3 | 58 | M | Unremarkable | HRVO | Bevacizumab (monthly) | 6/18 | ||
| 1st AZD1222 | 3 | 73 | F | HTN | BRVO | Aflibercept (monthly) | 6/19 | ||
| 1st BNT162b2 | 5 | 47 | F | Unremarkable | BRVO | Bevacizumab (monthly) | 6/9.6 | ||
| 2nd BNT162b2 | 1–3 | 36 | M | Unremarkable | CRVO | Aflibercept (monthly) | 6/9 | ||
| Sugihara et al. (Jan. 22) [20] | 1 | 2nd BNT162b2 | 11 L | 38 | M | Unremarkable | BRVO | Aflibercept*2 | 0.9->1.2 |
| Pur et al. (Feb. 22) [30] | 1 | 1st BNT162b2 | 2 R | 34 | M | Unremarkable | BRVO | None | 20/20 |
| Endo et al. (Sep. 21) [31] | 1 | 1st BNT162b2 | 15 L | 52 | M | Unremarkable | CRVO | Steroid*1 Bevacizumab*1 | 20/30->20/20 |
| Ikegami et al.(Nov. 2021) [21] | 1 | 2nd mRNA-1273 | 2 R | 54 | F | Unremarkable | CRVO + CRAO | None | NLP |
| Sacconi et al. (Dec. 2021) [22] | 1 | 2nd mRNA-1273 | 2 R | 74 | F | Unremarkable | HRVO | Ranibizumab*2 | 20/40->20/32 |
| Bialasiewicz et al. (Aug. 2021) [16] | 1 | 2nd BNT162b2 | 15 min L | 50 | M | Unremarkable | CRVO | Aflibercept | 0.5->1.0 |
| Park et al. (Dec. 2021) [23] | 11 | 1st AZD1222 | 1 L | 68 | F | Hyperlipidemia | RVO | None | HM |
| 1st BNT162b2 | 2 L | 76 | M | HTN | BRVO | None | 0.8 | ||
| 2nd BNT162b2 | 1 R | 85 | F | DM, HTN | RVO | Bevacizumab | CF10 | ||
| 1st AZD1222 | 2 L | 59 | M | DM, HTN | RVO | None | 0.8 | ||
| 1st AZD1222 | 2 R | 61 | M | Unremarkable | CRVO | Bevacizumab | 0.04 | ||
| 2nd BNT162b2 | 2 L | 79 | M | DM | RVO | Bevacizumab | 0.04 | ||
| 1st BNT162b2 | 16 L | 77 | F | HTN | BRVO | Bevacizumab | 0.8 | ||
| 1st BNT162b2 | 13 R | 63 | M | DM | RVO | Bevacizumab | 0.01 | ||
| 1st AZD1222 | 21 L | 51 | F | HTN | BRVO | Bevacizumab | 0.09 | ||
| 1st BNT162b2 | 4 L | 81 | F | HTN | RVO | None | 0.3 | ||
| 1st AZD1222 | 3 L | 61 | M | HTN | CRVO | None | 0.9 | ||
| Sonawane et al. (Dec. 2021) [24] | 2 | 2nd AZD1222 | 4 R | 50 | M | DM | CRVO | Anti-VEGF | 6/60 |
| 2nd AZD1222 | 3 R | 43 | F | Unremarkable | CRVO | None | 5/60 | ||
| Shah et al. (Dec. 2021) [32] | 1 | 1st BNT162b2 Worsen after 2nd | Few days | 27 | F | Unremarkable | CRVO | Ranibizumab | improved |
| Lee et al. (Jan. 2022) [25] | 1 | 2nd BNT162b2 | 10–12 L | 34 | M | Unremarkable | CRVO + CRAO + ischemic optic neuropathy | Aflibercept anti-inflammatories, diuretics, anti- platelet agents and anticoagulant | CF->20/30 |
| Sodhi et al. (June 2022) [33] | 1 | 1st AZD1222 | 3 L | 43 | M | Unremarkable | CRVO | Triamcinolone *1 | 20/630->20/200 |
| Romano et al. (July 2022) [26] | 1 | 2nd AZD1222 | 2 R | 54 | F | HTN | CRVO | Dexamethasone implant + PRP | 20/400 ->20/200 |
| Takacs et al. (Aug 2022) [34] | 1 | 1st BNT162b2 | 14 R | 35 | M | Unremarkable | CRVO | Aflibercept Oral aspirin | 0.5 ->1.0 |
| Karageorgiou et al. (Sep 2022) [35] | 1 | AZD1222 | 7 R | 60 | M | Unremarkable | BRVO | Anti-VEGF | - |
| Nangia et al. (Sep 2022) [36] | 1 | 1st Corbevax | 28 L | 13 | M | Unremarkable | CRVO | IVMP 0.5 g for 3 days followed by oral steroid | 6/7.5->6/6 |
| Majumder et al. (May 2022) [29] | 1 | 3rd AZD1222 | 25 R | 28 | M | Unremarkable | CRVO | IVMP 1 g for 3 days followed by oral steroid | 2/60->6/9 |
| Chen et al. (July 2022) [27] | 1 | 2nd BNT162b2 | 10 R | 72 | M | Unremarkable | CRVO + CRAO + exudative RD | Aflibercept IVMP 1 g for 3 days followed by oral steroid PRP | HM->20/400 |
| Vujosevic et al. (May 2022) [28] | 13 | 1st AZD1222 | 7 R | 69 | F | (Deep venous thrombosis) | BRVO | Laser photocoagulation | 20/32->20/20 |
| 2nd BNT162b2 | 14 R | 82 | F | Unremarkable | BRVO | Steroid treatment | 20/63->20/40 | ||
| 2nd BNT162b2 | 7 R | 96 | F | HTN, DM | CRVO | Steroid treatment | 20/200->20/200 | ||
| 2nd BNT162b2 | 10 L | 91 | F | Unremarkable | CRVO | None | CF | ||
| 2nd BNT162b2 | 7 both | 78 | F | Unremarkable | BRVO | Anti-VEGF, R | 20/25->20/20(R) 20/20(L) | ||
| 1st AZD1222 | 7 R | 70 | M | Unremarkable | CRVO | None | 20/20 | ||
| 1st AZD1222 | 14 R | 40 | M | Hyperhomocysteinemia | BRVO | None | 20/20 | ||
| 2nd BNT162b2 | 28 R | 91 | M | DM | BRVO | Steroid treatment | 20/32->20/32 | ||
| 2nd BNT162b2 | 21 R | 72 | F | HTN hyperlipidemia | BRVO | Steroid treatment | 20/25->20/20 | ||
| 2nd BNT162b2 | 14 R | 88 | M | HTN, hyperlipidema | HRVO | Steroid treatment | 20/125->20/125 | ||
| 2nd AZD1222 | 28 R | 73 | F | HTN, hyperlipidemia | CRVO | Steroid treatment | CF->CF | ||
| 1st Ad26. COV2 | 7 R | 65 | F | HTN, hyperlipidemia, DM | CRVO | Steroid treatment | 20/40->20/32 | ||
| 1st AZD1222 | 14 L | 72 | F | HTN | HRVO | Laser photocoagulation | 20/50->20/50 | ||
| Tanaka et al. (May 2022) [37] | 2 | 1st BNT162b2 | 3 R | 50 | F | Unremarkable | BRVO | Ranibizumab*3 | 20/25->20/20 |
| 1st BNT162b2 | 3 R | 56 | F | Unremarkable | BRVO | Ranibizumab*3 | 13/20->20/20 |
| Diagnosis | CRVO: 18 CRVO + CRAO: 1(mRNA-1273) CRVO + CRAO + ischemic ON: 1(BNT162b2) CRVO + CRAO + exudative RD: 1 (BNT162b2) |
| Sex | Male: 13 Female: 8 |
| Age | 13–96 |
| Vaccine | BNT162b2: 9 AZD1222: 9 mRNA-1273: 1 Ad26. COV2: 1 Corbevax: 1 |
| Onset after vaccination | 15 min to 28 days |
| Risk factors | HTN: 5 DM: 3 Hyperlipidemia: 1 |
| Treatment | IVI anti-VEGF (Aflibercept, Ranibizumab, Bevacizumab) and steroid, IVMP, laser photocoagulation |
| CRVO | BRVO | RVO | |
|---|---|---|---|
| Cases | 8 | 13 | 5 |
| Sex (Male/Female) | 5/3 | 7/6 | 3/2 |
| Age | 27–96(Average: 57) | 34–91(Average: 65) | 63–88(Average: 79) |
| Risk factors | 1 96 y/o patient and HTN and DM | HTN: 6 DM: 1 (deep vein thrombosis): 1 Hyperlipidemia: 1 Hyperhomocysteinemia: 1 | DM:4 HTN:5 Hyperlipidemia: 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sung, S.-Y.; Jenny, L.A.; Chang, Y.-C.; Wang, N.-K.; Liu, P.-K. Central Retinal Vein Occlusion in a Young Woman with Diabetes and Hypertension after mRNA-Based COVID-19 Vaccination—A Case Report and Brief Review of the Literature. Vaccines 2023, 11, 365. https://doi.org/10.3390/vaccines11020365
Sung S-Y, Jenny LA, Chang Y-C, Wang N-K, Liu P-K. Central Retinal Vein Occlusion in a Young Woman with Diabetes and Hypertension after mRNA-Based COVID-19 Vaccination—A Case Report and Brief Review of the Literature. Vaccines. 2023; 11(2):365. https://doi.org/10.3390/vaccines11020365
Chicago/Turabian StyleSung, Shao-Yu, Laura A. Jenny, Yo-Chen Chang, Nan-Kai Wang, and Pei-Kang Liu. 2023. "Central Retinal Vein Occlusion in a Young Woman with Diabetes and Hypertension after mRNA-Based COVID-19 Vaccination—A Case Report and Brief Review of the Literature" Vaccines 11, no. 2: 365. https://doi.org/10.3390/vaccines11020365